By Shelby Smoak, Ph.D.

A lyric from a favorite band of mine, Wilco, has always stuck out to me. When Jeff Tweedy sings, “I was saved by rock n’ roll,” I can’t help but think of all the ways rock ‘n roll has saved me.
It began with Billy Joel during my knee synovectomy at age 10. Music became the root for my recovery, and my growth throughout high school and college.
Music distracted me from self-infusion needle sticks and the half hours pushing in 60cc of clotting factor. It saved me from the pain of physical therapy when recovering from a total hip replacement, later a knee replacement, and from a traumatic month-long knee bleed. Music still saves me at 2 am when the pain of a bleed won’t let me sleep, or when I’ve been stuck in an ER for hours. And so, I let music save me, because it can, because no matter what pain I am in, nor what joy I may feel, it is there for me—always. I have come to realize my experience is not isolated. A plethora of our community members lean into music as their own, unique salvation: a balm to the hurt, a salve for the pain.
Through the BioMatrix Education program “Singing to Heal” which I often lead, I hear the same message about the power of music in other community members’ lives. Moreover, I am awed and impressed by the ways this suffering gets channeled into their musical creations, much like I do in my self-styled project, Bleeder, where memoir and music-creation blend. While we may not “write the songs that the whole world sings,” we may write the words our community can feel.
Without further ado, I invite you to check out this community playlist of original music from people with a bleeding disorder. It’s been a pleasure to hear their songs, to feel their power, and now, to share them with you.
“busting out the darkstar >country trux”
Billy Conde Goldman (creature-blossom)


Genre: Experimental; Harmolodic Rock ‘n’ Roll
For fans of: Mr. Bungle, Frank Zappa, Mike Patton
Shelby’s take: Atonal saxophone, a vocal cacophony of hypnotic and recurring lines, marching snare rolls, haphazard melodies, and fuzz guitar chords make this song a late-night, coffee-fueled journey into post-modernism.
On having hemophilia A: “Of all the songs I have written since I was a kid, only one mentions hemophilia in word. That said, many songs express pain, loneliness, sadness, fear and anger in the music and the lyrics—all a result of having a bleeding disorder. My sense is such expression would manifest in my songs no matter what, as life can be a struggle independent of wellness. Life can also be joyous and I have experienced much joy from being a part of the bleeding disorders community. This is also reflected in my songs.”
To Find: Search Google “creature-blossom busting out the darkstar”
“That’s When I Love Her So”
Dave Colvin

Genre: Country/Folk
For fans of: Beatles, John Prine, George Harrison

Shelby’s take: A bouncy acoustic guitar, catchy vocals, and playful lyrics make this upbeat love song a pared down, perfect for your coffee shop, mid-afternoon feel-good moment.
On having hemophilia A:
“Basically since prophylaxis treatment, having hemophilia doesn’t impact my music. Back in the day though when giving “as needed” treatment, performances were always problematic. Now I can plan ahead and give factor the day of a performance if needed!”
To Find: Search on Spotify and Apple Music: Dave Colvin That’s When
“Keeping Up”
Shawn Decker Co-written with Kyle Wiggins (Synthetic Division)

Genre: Electronic Dance Music
For fans of: Pet Shop Boys, Depeche Mode, New Order
Shelby’s take: Arpeggiated synthesizers, distorted synth-bass rhythms, driving EDM beats, a tasteful application of keyboard melodies, and understated vocals make this track the perfect late-night club companion.

On having hemophilia A: “Embracing every aspect of my life is important as a songwriter, and my bleeding disorder is certainly part of the equation. Finding peace through adversity has helped me deal with some tough situations medically, and I certainly draw upon that theme quite often in my music.”
To Find: Search on Spotify and Apple Music: Synthetic Division Keeping Up
“Lend Me a Hand”
Spencer Duggan (Skydiver)

Genre: Alternative Rock
For fans of: Radiohead, Elbow, Doves
Shelby’s take: A soft-strummed acoustic guitar, ultra-clean guitar licks, rolling bass lines, jazz-esque drum play; the drift of falsetto vocals carry the song along like the ebb and flow of a quiet city night, lending this song the ideal track for drinks and a rooftop bar.
On having hemophilia B: “Hemophilia played a large part in discovering my love for music. It is a great way to reset my mind even when things are hard. I consider myself lucky to have it under control so I can keep making music for myself and my local chapter for years to come.”
To Find: Search on Spotify and Apple Music: Skydiver Lend Me a Hand
“Spratz”
Max Feinstein

Genre: Alternative Rock/Grunge
For fans of: Ween, Fountains of Wayne, Radiohead (Bends-era)
Shelby’s take: Infectious distorted guitar riffs, fluid bass lines, a driving chorus, energized vocals, and amazing studio production make this song a pool party instant hit.

On having hemophilia A:
“Joint damage makes it physically difficult to play and has influenced the stylistic aspects of my songwriting. In addition to producing spontaneous bleeds, hemophilia can produce a lot of rage. We don’t want that rage to bleed out into the wrong places, much like bleeding into the wrong places. Music was the safest place to channel my aggression and in doing so, it became catharsis.”
To Find: Search on Spotify and Apple Music: Max Feinstein Spratz
“Remnants”
Trevor Graham (Organ Dealer)

Genre: Punk/Grindcore
For fans of: Napalm Death, PLF, Death Toll 80K
Shelby’s take: Adrenaline fueled angst, thick chugging guitars, propulsive bass lines, snare hits faster than you can clap, and screaming, deep throated vocals thrust this song at you; for half a minute, the song clobbers you with its punk-on-steroids energy.

On having hemophilia A:
“It makes touring a little difficult sometimes, lots of standing which impacts the joints, then [there is] the trouble of finding a place to infuse.”
To Find: Search on Spotify and Apple Music: Organ Dealer Remnants
“You are Not Alone”
John Harrison (Jphono1)

Genre: Alternative/Indie Rock, Jamz
For fans of: Flaming Lips, Pink Floyd, Kurt Vile
Shelby’s take: Chill groove, in the pocket bass, 70s-feel guitar lines, fuzzed-out playful organ lines, and Pink Floyd-esque vocal delivery makes this a perfect sunshine, porch-time play.
On having hemophilia B:

“It’s not a daily concern but have had internal bleeds that have forced me to cancel live events. Hospital visits and making sure there is factor in my fridge for emergencies. Creatively, it’s such a small part of my life it doesn’t come into play... but I imagine it’s in there in some ways I couldn’t identify.”
To Find: Search YouTube: jphono1 You are Not Alone
“Go-To”
Trevor Martin

Genre: Pop Country
For fans of: Kane Brown, Dan + Shay, Brett Young
Shelby’s take: Rolling piano lines, country-telecaster licks; immediate and intimate vocals, the incredibly hooky “Go-To” refrain lands this song somewhere between country ballad and R&B. A supreme listen for driving with your windows down and your hair blowing in the country breeze.

On having hemophilia A:
“Having hemophilia really impacted me earlier on in life. It helped me discover that I really enjoy and have a passion for music. I am not sure I would have discovered that as quickly had I been playing football or another sport.”
To Find: Search on Spotify and Apple Music: Trevor Martin Go-To
“No Way Josè”
Robb McDowell (Louisville Lip)

Genre: Punk/Alternative Rock
For fans of: Social Distortion, Bad Religion, The Stooges

Shelby’s take: Distorted guitars, thudding basslines, locked-in pounding drums; throaty vocals with vitriolic angst drive this song into a high-energy, cathartic vent – ideal for blasting on a warm summer night classic car ride – top down, open and free.
On having hemophilia B: Having a bleeding disorder is probably one of the main reasons I got into writing music among other things. It’s a way for me to express my mood and how I’m feeling. I’ve never been one to talk about “feelings” so this was the best way for me to get things out.
To Find: Search on Spotify and Apple Music: Louisville Lip No Way Jose
“Be Mine”
Tamar Mitchel

Genre: R & B / Pop
For fans of: Justin Bieber, Chris Brown, Justin Timberlake

Shelby’s take: Hip-hop beats dipping into classic 808 tones, a catchy repetitive guitar line, a head-nod bpm, and tripped out vocals make this song a smooth ride for a late evening city stroll. Mixing soulful R & B with modern electronica carries this tune into sultry perfection.
On having hemophilia A:
“Having hemophilia impacts my music by helping me have the drive to want better for myself and my family. It pushes me to be my best possible self and in doing so, helping others.”
To Find: Search on Spotify and Apple Music: Tamar Mitchell Be Mine
“A Collection of British Invasion Hits”
Bobby Murdoch (The British Invasion Years)

Genre: 1960s Rock
For fans of: The Beatles, The Who, The Zombies

Shelby’s take: The nostalgia of jangling guitars, bouncing bass lines, psychedelic keyboards, and familiar lyric sing-alongs make this cover band the ideal live show flashback. Infused with psychedelic hearts, these cover songs nail the 1960s vibe and ooze groovy, mind-bending bliss.
On having hemophilia A:
“Music has always been a way to forget about my bleeding disorder. It also motivates me to continue performing.”
To Find: Visit britishinvasionyears.com and click Videos
“Glide”
Cleaven Pagani

Genre: Alternative
For fans of: Radiohead, Elliott Smith

Shelby’s take: Delicate guitar picking, tasteful keyboard subtexts, and whisper-intimate vocals that ponder the burdens of life make this trimmed down song the end-of-night, goodnight, best-friend companion.
On having hemophilia A:
“I write songs about my life, which includes living with a bleeding disorder. With this song, I attempt to describe how we glide through life encountering many crazy things. It could be a bleeding disorder, psychological illness, divorce, or other situation. We all have burdens to bear that can be unexpected and terrible, but everything is okay when we have someone we love with us.”
To Find: Search Bandcamp: Cleaven Pagani, Click Stargazer, 1st track
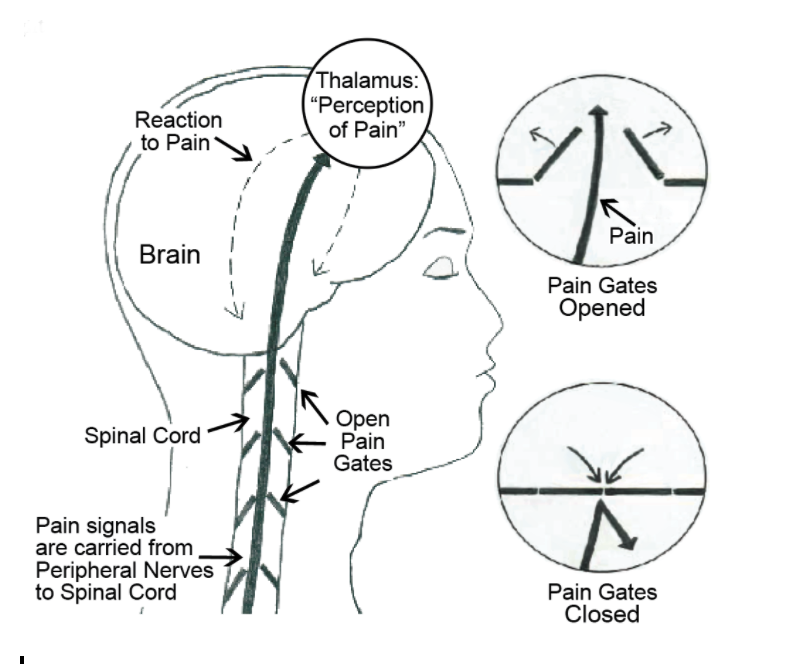
“Pain”
Shelby Smoak (Bleeder)

Genre: Alternative Rock/Shoegaze
For fans of: Radiohead, The Cure

Guest reviewer’s take: A medley of sound with a mixture of new wave alternative, grunge, rock, and indie. Sweet guitar intro with melodic back vocals and smooth bass guitar transitions into a blend of guitar and toe-tapping percussion and fills. The lyrics and message are unmistakable as it not only relates to those with a bleeding disorder but can resonate with anyone living with pain.
On having hemophilia B:
“Music has always been a solace for me. It comforts when nothing else can. Writing music does the same thing. A song like ‘Pain’ gives voice to something hard to articulate: living with the chronic pain of hemophilia.”
To Find: Search on Spotify and Apple Music: Bleeder Pain
Stay informed on the latest trends in healthcare and specialty pharmacy.
Sign up for our monthly e-newsletter, BioMatrix Abstract.
By giving us your contact information and signing up to receive this content, you'll also be receiving marketing materials by email. You can unsubscribe at any time. We value your privacy. Our mailing list is private and will never be sold or shared with a third party. Review our Privacy Policy here.